
Barriers to services
– and how to remove them
SAFEGUARDING FOUNDATIONS

Kā i te wā mātau ai tāngata, kā whai kaha.
When people are aware, they are strengthened.
Since 2024, VisAble has been funded by the Centre for the Prevention of Family Violence and Sexual Violence (the Centre) to undertake “Community engagement to address system barriers for disabled people and tāngata whaikaha Māori experiencing family and sexual violence”.
VisAble has been facilitating this mahi (work) through its Kaitiakitanga te Hāpori / Disability Community Kōrero approach.
Hui and kōrero (workshops, meetings and conversations) are being held in various centres across Aotearoa New Zealand, involving tāngata whaikaha Māori and disabled people and their whānau (family members).
A draft report has been prepared for the Centre, for use in advocating for change. Once completed, the report will be available through the centre and published on VisAble’s website.


In summary, the findings show that:
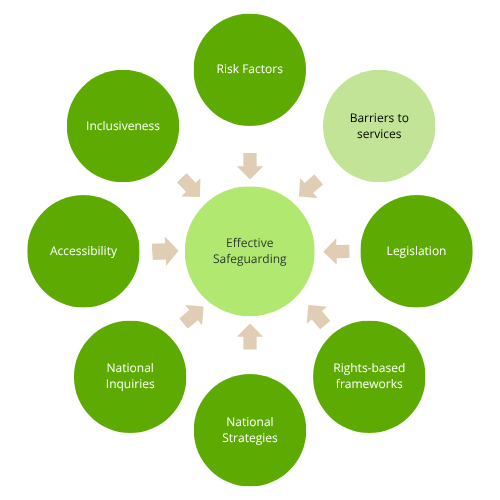
Disabled people and tāngata whaikaha Māori typically experience six key barriers to accessing family violence and sexual violence services.
There are five key recommendations for the Centre to share with government and service providers.
The findings are outlined below, and you can also download a factsheet here.

Supplementing these findings are insights gained through recent disability community consultations on the refreshed New Zealand Disability Strategy (NZDS) and the Royal Commission of Inquiry into Abuse in State Care and in the Care of Faith Based Institutions (AIC).
Together, these consultations have involved thousands of voices.

Summary of Barriers and Recommendations
Kaitiakitanga te Hāpori – Community Engagement Findings
This summary outlines the key systemic barriers experienced by tāngata whaikaha Māori and disabled people in relation to family violence and sexual violence (FVSV), and the recommendations identified as a result.
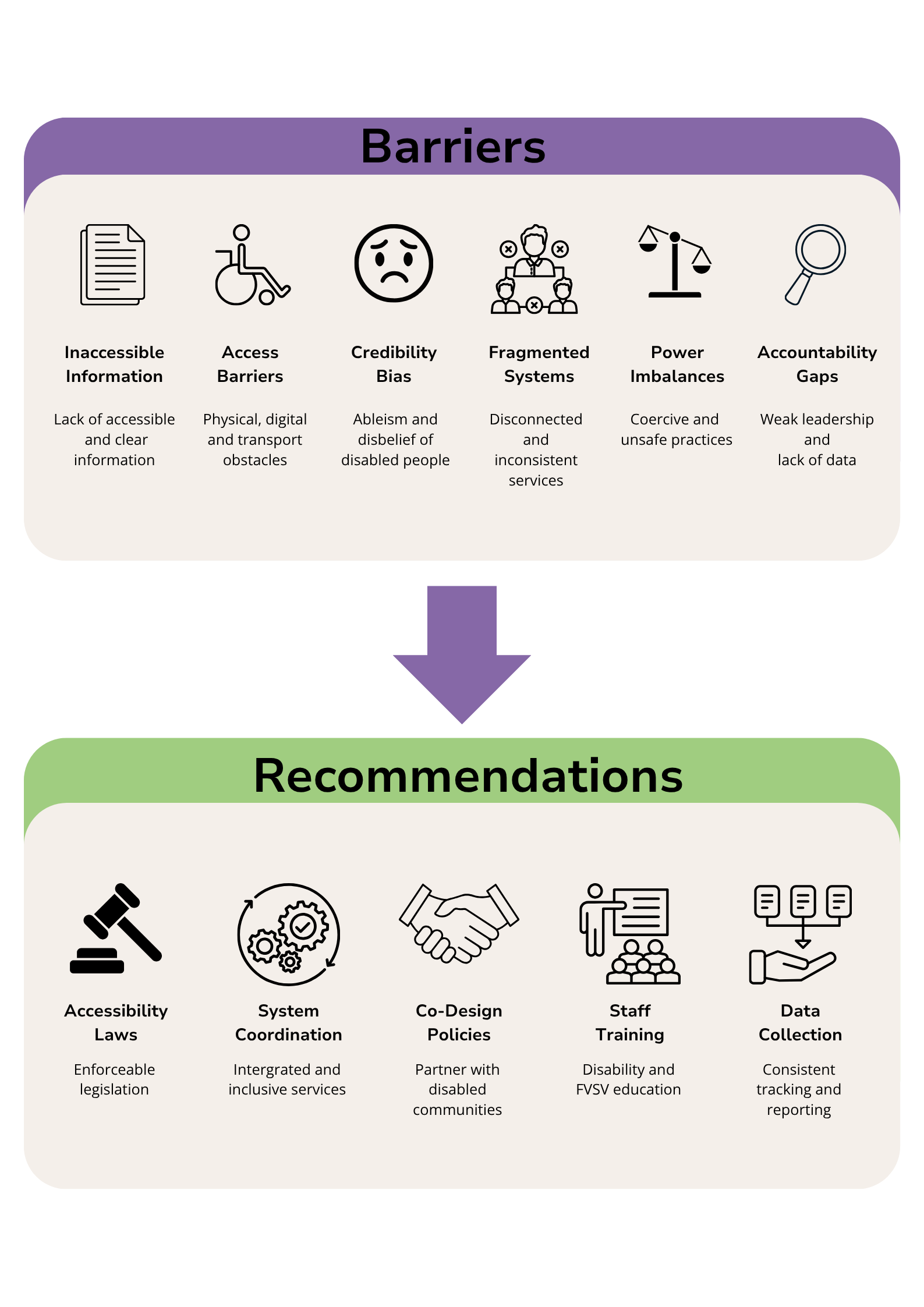
Barriers
The findings identified six barriers typically experienced by disabled people when seeking FVSV services:
-
Information about family violence and sexual violence (FVSV), people’s rights, and what kinds of services isn’t often provided in accessible formats (such as Easy Read, New Zealand Sign Language [NZSL], visual communication, or even plain language).
When information is complex, or hard to find, understand and use, it becomes harder for:
violence, abuse or neglect to be identified or detected
people to feel safe about reporting harm
people to know where to go for support
informed consent to be obtained
safe disclosures to be made (this means people being abused, or at risk of abuse, feeling safe to tell someone about the abuse)
harm being recognised by the person being abused (for example, when the abuse has been normalised, or perhaps carried out by a family member or by someone in authority, whose actions aren’t questioned).
-
Accessibility is often treated by service providers as optional rather than a core safeguarding requirement.
Evidence shows that there are many barriers that can prevent or limit access to help. These barriers can be:
Physical: such as access to buildings being via stairs rather than ramps, lack of accessible toilets, swing doors rather than sliding doors.
Sensory: where services are provided in areas that are too busy, too crowded, too noisy or too brightly lit for some neurodivergent people.
Digital: requiring access to computers, laptops, smart phones or other technology, and requiring skills and confidence in using online and digital formats.
Transport-related: lack of public transport or ability to pay for a taxi or hired car to get to services.
Procedural: too many actions or tasks required by the service provider or organisation, or confusion about what’s required to support any request for help (especially when dealing with a different staff member each time or if you’re asked to provide different information each time).
Practice-based: organisations or professionals not being aware of or equipped for disabled people’s personal needs (for example, people with learning disabilities might need extra time to process information and discuss what’s happening; a Deaf person might need NZSL; a person with English as a second language might need access to a translator).
Psychological: people not feeling safe to raise or discuss the violence, abuse or neglect they’re experiencing, or feeling too ashamed to tell someone else.
These barriers are often even greater (more prevalent) in regional and rural communities due to distance, lack of services, and people’s lack of access to online systems or tools (such as computers and laptops) – or the lack of privacy, in a small community.
-
Attitudinal ableism and credibility bias
When trying to share their real and valid experiences of harm or abuse, disabled people are frequently disbelieved, or pathologised (meaning their experiences are treated as symptoms of their impairment or mental health – rather than as actual situations, they’re experiencing), or they find that their experiences are minimised.
Abuse is reframed as “care issues” or as a misunderstanding, minimising the situation and the need to understand and address what’s happening.
Assumptions are often made about the person’s capability, parenting / caregiving, or communication – and these also minimise the situation and reduce safety and trust.
-
Services (for disability, FVSV, health, justice, and housing) operate in silos and with poor inter-agency co-ordination.
Survivors must repeatedly retell trauma to different organisations, and to different people within organisations, which creates a significant barrier for them in seeking support. Having to repeatedly tell their story, re-traumatises people who have experienced abuse.
Often the responsibility for navigating complex systems or requirements, both within and across government agencies or other service providers, is pushed onto those people needing support, leaving them feeling isolated, confused, frustrated, misunderstood and incapable.
Systems prioritise process and compliance (i.e. the need to meet the organisation’s or system’s requirements) over the disabled person’s dignity and safety.
-
Communication supports, information, or services are withheld, used coercively, or are inconsistently provided. (“Used coercively” means supports or services are used to pressure, control, or influence a person, rather than to support their rights, safety, and enable an informed choice).
Complaints pathways are often difficult to access and can be intimidating or ineffective.
Disabled people experience the system as unsafe, unhelpful, unfair or punitive.
-
Weak or unclear leadership responsibilities within organisations reduce people’s follow-through and trust.
The lack of ‘disability-specific FVSV data’ limits organisational insights and understanding, and prohibits (stops) system-based planning. This impacts the effectiveness of systems for disabled people.
Historic consultation fatigue heightens scepticism. This means that some disabled people feel that, in the past there’s been a lot of consultation – to the point that people get tired of being asked – and especially as they also feel that nothing comes of seeking their views. They don’t feel heard, they don’t see the results of their input, and therefore they don’t feel respected.
Recommendations for removing these barriers – for government agencies and service providers
The findings identified five key areas for action in removing barriers:
-
Develop comprehensive, enforceable accessibility legislation with clear compliance mechanisms.
Consolidate relevant legislation in one location.
Address gaps in protections for disabled adults aged 18–65.
Strengthen complaints and compensation processes.
-
Make accessibility a core requirement in all government contracts.
Ensure all information is released in accessible formats by default.
Strengthen regional service availability - and reduce digital exclusion.
Improve inter-agency communication and co-ordinated pathways to reduce ‘passtheparcel’ experiences.
Collect consistent data on disabled peoples’ interactions with FVSV services.
Embed tāngata whaikaha Māori and disabled people in FVSV planning and decision-making, so that co-design can enable improvements and effectiveness.
-
Organisations should:
Co-design accessibility policies with disabled people and tāngata whaikaha Māori.
Provide ongoing staff training on accessibility, disability rights, and FVSV responsiveness.
Build strong partnerships with NZSL interpreters, disability services, and supported decision-making specialists.
Develop organisational disability strategies and succession planning to maintain capability over time.
-
Presume that disabled people are competent and ensure that their lived experience is ‘front and centre’ in all interactions.
Provide regular cultural supervision for staff that has a disability-lens.
Improve visibility of accessible communication for disabled people (e.g. Easy Read versions and NZSL need to be obvious and very easy to access and use, in digital communications – put these first).
Strengthen relationships between disability and FVSV sectors.
Ensure FVSV and disability workers have ongoing training in prevention, communication, and responsiveness.
-
Strengthen oversight bodies such as the Human Rights Commission and Health and Disability Commissioner.
Introduce enforceable consequences for failure to meet accessibility obligations.
Establish clear, mandated pathways for action and follow-up.
Support organisations to improve accessibility practices and reduce transition fatigue for disabled people who need to work with more than one agency, or more than one staff member.
For your action:
Reflect on the barriers to services and to what extent these are occurring in your organisation or practice.
Watch the video below and consider how you can create change and uphold the social model of disability in your organisation and practice.
Read the related material on Accessibility and Inclusiveness
Ask disabled people what their experience is like, in accessing your services.
Identify at least two areas you can improve - and set a timeframe for achieving this.
Enlist the support of your leaders and/or your team.
Create an action plan, and track your organisation’s progress and achievements:
so that you’re actively addressing one or more identified barrier very 3-6 months.
The social model of disability
Your organisation or practice might be familiar with (and perhaps unconsciously using) the medical model of disability, when interacting with disabled people. That model is now outdated in a safeguarding context.
This video outlines the social barriers that disable people, and how the social model of disability provides opportunities to build a more equal society.
Produced by the National Disability Arts Collection and Archive (NDACA) and Shape Art, UK, 2019